Healthcare in the United States of America

Healthcare related pages on Justice Network
On Health Care, We’ll Have What Congress Is Having

On Health Care, We’ll Have What Congress Is Having
The New Yorker
By Jeffrey Frank
January 17, 2017
In the fall of 1994, the Clinton Administration’s much debated comprehensive, and complicated, health-insurance bill—known derisively as Hillarycare—died quietly on Capitol Hill. It was a moment that, the Princeton sociologist Paul Starr later argued, would "go down as one of the great lost political opportunities in American history." But, before the end, talk of another approach kept bubbling up: to allow those Americans who couldn’t get insurance elsewhere to buy a policy that was just as good, and inexpensive, as what members of Congress got. When Senator Edward M. Kennedy, of Massachusetts, said that Americans should get "exactly what we have," he meant the Federal Employees Health Benefits Program.
The F.E.H.B.P., as it’s known, was started in 1959, a few years before Medicare, and was meant to cover some nine million government employees—civil-service workers, the courts, the Post Office, members of Congress, and more. It wasn’t a single plan but, rather, as a Times story put it, "a supermarket offering 300 private health plans." (Even the right-learning Heritage Foundation called it "a showcase of consumer choice and free-market competition.") One may get a sense of its scope and inclusiveness—its supermarket-ness—in the way that the Office of Personnel Management, which administers the program, explains it to federal employees. Much of the program—for instance, the idea that no one can be refused, or charged more, for a preëxisting condition, or that dependents under twenty-six are covered—will sound familiar to anyone conversant with the most attractive parts of the Affordable Care Act. Read more
Federal Employees Health Benefits Program

Federal Employees Health Benefits (FEHB) Program Official Website
FEHB Program Overview PDF
FEHB Program Benefit Details
FEHB Program YouTube Video1
FEHB Program YouTube Video2
Report on Health Information Technology (HIT) and Transparency
Laws Affecting the Federal Employees Health Benefits (FEHB) Program Congressional Record Service PDF July 22, 2015

- Congress ObamaCare:
- ObamaCare Exemption for Congress?
The ObamaCare Exemption for Congress is a myth. It turns out that reports that members of Congress will be exempt from ObamaCare are without merit. Members of Congress have to buy their health insurance on the exchanges along with millions of other Americans.
 www.factcheck.org/2009/08/health-care-for-members-of-congress/
www.factcheck.org/2009/08/health-care-for-members-of-congress/
- Health Care for Members of Congress?
- FactCheck.org (correction of old information)
For a full discussion of current health insurance options for members of Congress, see the 2017 Congressional Research Service paper "Health Benefits for Members of Congress and Designated Congressional Staff: In Brief.
Before the ACA, "House and Senate members are allowed to purchase private health insurance offered through the Federal Employees Health Benefits Program, which covers more than 8 million other federal employees, retirees and their families." "It’s not a "single-payer" system where the government acts as the one and only health insurance company." Read more

Federal Employees Health Benefits Program Wikipedia
The Federal Employees Health Benefits (FEHB) Program is a system of "managed competition" through which employee health benefits are provided to civilian government employees and annuitants of the United States government. The government contributes 72% of the weighted average premium of all plans, not to exceed 75% of the premium for any one plan (calculated separately for individual and family coverage).[1]
The FEHB program allows some insurance companies, employee associations, and labor unions to market health insurance plans to governmental employees. The program is administered by the United States Office of Personnel Management (OPM). Read more
President Trump Healthcare Listening Session transcript
President Trump Healthcare Listening Session video
Medicare (United States)
Medicare (United States)
Wikipedia
In the United States, Medicare is a single-payer, national social insurance program administered by the US federal government since 1966, currently using about 30–50 private insurance companies across the United States under contract for administration.[1] United States Medicare is funded by a payroll tax, premiums and surtaxes from beneficiaries, and general revenue. It provides health insurance for Americans aged 65 and older who have worked and paid into the system through the payroll tax. It also provides health insurance to younger people with some disabilities status as determined by the Social Security Administration, as well as younger people with end stage renal disease and amyotrophic lateral sclerosis.
In 2015, Medicare provided health insurance for over 55 million—46 million people age 65 and older and nine million younger people.[2] On average, Medicare covers about half of the health care charges for those enrolled. The enrollees must then cover their remaining costs either with supplemental insurance, separate insurance, or out-of-pocket. Out-of-pocket costs can vary depending on the amount of health care a Medicare enrollee needs. They might include the costs of uncovered services—such as for long-term, dental, hearing, and vision care—and supplemental insurance premiums.[3]
The Specialty Society Relative Value Scale Update Committee (or Relative Value Update Committee; RUC), composed of physicians associated with the American Medical Association, advises the government about pay standards for Medicare patient procedures performed by doctors and other professionals under Medicare Part B, according to news reports.[4] A similar but different CMS system determines the rates paid acute care and other hospitals—including skilled nursing facilities—under Medicare Part A. more

Letter: The real value of Medicare
Memphis Commercial Appeal
by Arthur J. Sutherland III, M.D.
January 9, 2012
Gerald Friedman, a professor of economics at the University of Massachusetts-Amherst, made this comment last summer on the Dollars & Sense: Real World Economics
website:
"America's broken health care system suffers from what appear to be two separate problems. From the right, a chorus warns of the dangers of rising costs; we on the left
focus on the growing number of people going without health care because they lack adequate insurance. ... But the division between the problem of cost and the problem of coverage is misguided. It is
founded on the assumption ... that the current market system is efficient. Instead, however, the current system is inherently inefficient; it is the very source of the rising cost pressures. In fact,
the only way we can control health care costs and avoid fiscal and economic catastrophe is to establish a single-payer system with universal coverage." Read more
Blue Cross Blue Shield Association

Blue Cross Blue Shield Association
Wikipedia
The Blue Cross Blue Shield Association (BCBSA) is a federation of 36 separate United States health insurance organizations and companies, providing health insurance to more than 106[1] million Americans.[1] Blue Cross was founded in 1929, and became the Blue Cross Association in 1960, while Blue Shield emerged in 1939 and the Blue Shield Association was created in 1948. The two organizations merged in 1982. Read more
Did Blue Cross' Mission Stray When Plans Became For-Profit?

Did Blue Cross' Mission Stray When Plans Became For-Profit?
National Public Radio - NPR
By Sarah Varney
SARA VARNEY: It may be hard to imagine now, but back in the 1930s, membership in a Blue Cross plan was practically a civic duty. Boy Scouts handed out enrollment brochures and preachers urged their congregation to enroll.
Blue Cross and Blue Shield plans formed as not-for-profits to give communities access to medical care and protect against personal financial ruin. All members paid the same amount no matter how old or sick, and no one was turned away. The Blues became one of the most trusted brands in America.
Mr. FAHEY FLYNN (News Anchor): How do you do, ladies and gentlemen? I'm Fahey Flynn with tonight's CBS News Special, brought to you as a public service by Blue Cross and Blue Shield. And to bring us up...
VARNEY: By the 1970s and '80s, though, Blue plans faced competition from for-profit insurance companies. Because the Blues accepted all comers, regardless of health status, their rates were typically higher. These new insurers who didn't offer universal coverage attacked younger, healthier people with better deals. In response, most Blue plans started charging sicker and older people more. Even so, Blue plans around the country were losing market share.
Ms. LAURIE SOBEL (Attorney, Consumers Union): There was basically mounting pressure from the plans that wanted to become for-profit. Read more
Expanded & Improved Medicare for All Act

Expanded & Improved Medicare for All Act
Introduced in House (01/24/2017)
Sponsor: Rep. John Conyers Jr. (D)
This bill establishes the Medicare for All Program to provide all individuals residing in the United States and U.S. territories with free health care that includes all medically necessary care, such as primary care and prevention, dietary and nutritional therapies, prescription drugs, emergency care, long-term care, mental health services, dental services, and vision care. Read more
Recent History of House Medicare for All bills
H.R.676 - Expanded & Improved Medicare For All Act
115th Congress (2017-2018)
Sponsor: Rep. John Conyers Jr. (D) Michigan’s 13th District
H.R.1200 - American Health Security Act of 2015
114th Congress (2015-2016)
Sponsor: Rep. Jim McDermott (D) Washington’s 7th District
H.R. 676 - Expanded & Improved Medicare For All Act
113th Congress 2013–2015
Sponsor: Rep. John Conyers Jr. (D) Michigan’s 13th District
Physicians for a National Health Program (PNHP)
 http://www.pnhp.org/
http://www.pnhp.org/
 www.pnhp.org/nhi
www.pnhp.org/nhi
 http://pnhp.org/blog/2013/07/31/friedman-analysis-of-hr-676-medicare-for-all-would-save-billions/
http://pnhp.org/blog/2013/07/31/friedman-analysis-of-hr-676-medicare-for-all-would-save-billions/
Physicians for a National Health Program (PNHP)
Physicians for a National Health Program (PNHP) is a non-profit research and education organization of 20,000 physicians, medical students and health professionals who support single-payer national health insurance.
PNHP reports Analysis of HR 676: Medicare for All would save billions, Physicians for a National Health Program, by Gerald Friedman, Ph.D. "Of all the forms of inequality, injustice in health care is the most shocking and inhumane." Martin Luther King, Jr.


The business case for single payer
Fix It Healthcare.com
Business owner Richard Master knows firsthand how the dysfunctional U.S. health care system punishes not only patients, but also employers who are forced to spend more and more to insure their workers. His documentary, "Fix It," makes a strong business case for addressing this festering problem, and includes interviews with many PNHP members. A trailer for the film can be accessed above, or you can view the full version for free by visiting the "Fix It" website. Read more
- Fix It Healthcare - Get Active HERE!
- Fix It Healthcare - Watch the Movie
- Fix It Healthcare brochure booklet PDF
- Fix It Healthcare tri fold brochure PDF
The Only Way to Win Single Payer is to Leave the Democratic Party - BAR Executive Editor Glen Ford

The Only Way to Win Single Payer is to Leave the Democratic Party
A Black Agenda Radio commentary by executive editor Glen Ford
"Not one Democratic Senator is committed to single payer. That includes Bernie Sanders, who has not submitted a bill this year – and, if you don’t have a bill, then you’re not serious about single payer health care. Sanders talked up a storm about single payer during the primary campaign, but then essentially shut up after endorsing Hillary Clinton, the candidate who said that single payer would "never, never" happen. That wasn’t a prediction; it was a promise by Clinton that she would do her utmost to prevent health care from becoming a right in the United States." Read more

Single-payer healthcare
Wikipedia
Single-payer healthcare is a system in which the state, rather than private insurers, pays for healthcare costs.[1] Single-payer systems may contract for healthcare services from private organizations (as is the case in Canada) or may own and employ healthcare resources and personnel (as is the case in the United Kingdom).
The term "single-payer" thus describes the funding mechanism, referring to healthcare financed by a single public body from a single fund, not the type of delivery or for whom physicians work. The British system is technically not single-payer, as it consists of a number of financially and legally autonomous trusts and private health insurance options are also allowed. Only Canada and Taiwan have true single-payer systems.[2]
The actual funding of a "single-payer" system comes from all or a portion of the covered population. Although the fund holder is usually the state, some forms of single-payer use a mixed public-private system. Read more
How and Why Medicare for All Is a Realistic Goal

By Nancy Altman
Founding Co-director
Social Security Works
Hillary Clinton is wrong when she says that Medicare for all is not achievable. In fact, if she and her husband had embraced the concept in 1993, we would be nearly there today.
Medicare was supposed to be a first step toward Medicare for all. After activists tried and failed to include universal health care in the Social Security Act of 1935, and after President Harry Truman tried during his presidency to achieve that goal, supporters decided that an incremental approach was most likely to bring ultimate success. Read more
Healthcare Reform In The United States of America

Health care reform in the United States has a long history, including two federal statutes enacted in 2010: the Patient Protection and Affordable Care Act (PPACA), signed March 23, 2010, also called Obamacare, and the Health Care and Education Reconciliation Act of 2010 (H.R. 4872 ), which amended the PPACA, March 30. Wikipedia
- History of health care reform in the US Wikipedia
- Health Care Reform Subject Directory NY Times
United States Health Care Reform: Progress to Date and Next Steps. National Institutes of Health, by B. Obama
United States Health Care Reform: Progress to Date and Next Steps. The JAMA Network, by Barack Obama, JD
The JAMA Network, by Barack Obama, JD
jama_Obama_2016_sc_160013.pdf
Adobe Acrobat document [624.7 KB]
 http://www.pnhp.org/beyondaca
http://www.pnhp.org/beyondaca

U.S. Health Care Reform Will Require Politicians to Change Their Attitude
Harvard Business Review
Health Care Reform Subject Directory
US News & World Report
History of Health Reform PDF, Kaiser Family Foundation
A Brief History on the Road to Healthcare Reform: From Truman to Obama, Becker’s Hospital Review
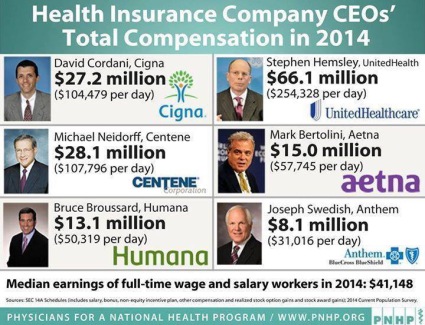 http://www.pnhp.org/news/2014/june/skyrocketing-salaries-for-health-insurance-ceos
http://www.pnhp.org/news/2014/june/skyrocketing-salaries-for-health-insurance-ceos

Medicare for All
Astronomical healthcare costs and lack of access continue to drive individuals, families and businesses past their breaking point while insurance companies continue to soak-up billions of healthcare dollars as millions of children's basic needs go unmet.
NNU supports the American Health Security Act of 2015, H.R. 1200 and the Expanded & Improved Medicare For All Act, H.R. 676, that requires each participating state to set up and administer comprehensive healthcare services as an entitlement for all, through a progressively financed, single-payer system, administered by the states.
Medicare has provided guaranteed healthcare for millions of American seniors, marks its 50th anniversary this year. The American Health Security Act, H.R. 1200 and H.R. 676, would establish a Medicare for all, single-payer healthcare system that would end health disparities, effectively control costs, and assure that everyone has equal access to an excellent standard of care.

'When It Matters Most, Insist on a Registered Nurse'
Nurses Launch New Campaign to Alert Public to Dangers of Medical Technology and Erosion of Care Standards
Sweeping changes underway in the nation’s health care delivery system that expose hundreds of thousands of patients to severe risk of harm are the focus of a major new national campaign by the nation’s largest organization of nurses announced today. —National Nurses United, 05/13/14 more
Bernie Sanders: ‘I Am Prepared to Run for President of the United States’ The Nation, March 6, 2014, by John Nichols
Bernie Sanders: I Would Be A Better President Than Hillary Clinton, The Huffington Post, March 5, 2014, by Mollie Reilly
The Patient Protection and Affordable Care Act; also known as Obama Care - currently the law of the land

The Patient Protection and Affordable Care Act
- Link to summary report, Democrats.Senate.Gov/Reform
- Patient Protection and Affordable Care Act (908page PDF)
- H.R.3590 - Patient Protection and Affordable Care Act
- Affordable Care Act, U.S. Department of Labor website
- Affordable Care Act, HealthCare.Gov
Patient Protection and Affordable Care Act, Wikipedia
The Patient Protection and Affordable Care Act (PPACA) is a United States federal statute that was signed into law by President Barack Obama on March 23, 2010. The law (along with the Health Care and Education Reconciliation Act of 2010) is a product of the health care reform agenda of the 111th United States Congress and the Obama administration. The PPACA reforms certain aspects of the private health insurance industry and public health insurance programs, including increasing insurance coverage of pre-existing conditions and expanding access to insurance to over 30 million Americans. Read more
2014 Update, Will the U.S. Supreme Court Destroy the Affordable Care Act? Melissa Harris-Perry, The Nation, November 12, 2014

 Devon Campbell-Williams, an inmate in OR, will have insurance for the first time under the Act
Devon Campbell-Williams, an inmate in OR, will have insurance for the first time under the Act
Prisons and jails signing inmates up for health insurance under the Affordable Care Act
American Bar Assocciation
ABA Journal Law News Now
by Mark Hudson
March 10, 2014
Prisons and jails are taking advantage of the expansion of Medicaid under the Affordable Care Act and signing their inmates up for health insurance.
The law lets states extend coverage to single and childless adults—a major part of the prison population, the New York Times reports.
Medicaid does not cover standard health care for inmates, but it can pay for hospital stays longer than 24 hours. Inmates enrolled in Medicaid while incarcerated can
also have coverage after they get out, the story says.
People coming out of prison have disproportionately high rates of chronic diseases, such as mental illness and addictive disorders. And many of them would qualify for
Medicaid under the income test of the program in the 25 states that have expanded it, the story notes. Read more
- Little-Known Health Act Fact: Prison Inmates Are Signing Up The New York Times, By ERICA GOODE, March 9, 2014
Sicko | Documentary | Michael Moore

Sicko (Wikipedia) is a 2007 American political documentary film by filmmaker Michael Moore. Investigating health care in the United States, the film focuses on the country's health insurance and the pharmaceutical industry. Moore compares the for-profit non-universal U.S. system with the non-profit universal health care systems of Canada, the United Kingdom, France and Cuba. Read more

FRONTLINE Sick Around America

FRONTLINE | Sick Around America | PBS
Introduction March 31, 2009
As the worsening economy leads to massive job losses—potentially forcing millions more Americans to go without health insurance—FRONTLINE travels the country examining
the nation's broken health care system and explores the need for a fundamental overhaul. Veteran FRONTLINE producer Jon Palfreman dissects the private insurance system, a system that not only fails
to cover 46 million Americans but also leaves millions more underinsured and at risk of bankruptcy. Read more
By T.R. Reid
A New York Times Bestseller, with an updated explanation of the 2010 Health Reform Bill
Bringing to bear his talent for explaining complex issues in a clear, engaging way, New York Times bestselling author T. R. Reid visits industrialized democracies around the world–France, Britain, Germany, Japan, and beyond–to provide a revelatory tour of successful, affordable universal health care systems. Now updated with new statistics and a plain-English explanation of the 2010 health care reform bill, The Healing of America (author site) is required reading for all those hoping to understand the state of health care in our country, and around the world. Read more
Washington Post Book Review: The Healing of America by T.R. Reid
T. R. Reid’s newest book, A Fine Mess, is forthcoming from Penguin Press. 9 Books On Healthcare For People Wanting To Fix Healthcare
Founding Fathers favored government run health care
 President John Adams
President John Adams
Newsflash: Founders favored "government run health care"
The Washington Post
By Greg Sargent
January 20, 2011
Forbes writer Rick Ungar is getting some attention for a piece arguing that history shows that John Adams supported a strong Federal role in health care. Ungar argues that Adams even championed an early measure utilizing the concept
behind the individual mandate, which Tea Partyers say is unconsittutional.
I just ran this theory past a professor of history who specializes in the early republic, and he said there's actually something to it. Short version: There's no proof
from the historical record that Adams would have backed the idea behind the individual mandate in particular. But it is fair to conclude, the professor says, that the founding generation supported
the basic idea of government run health care, and the use of mandatory taxation to pay for it.
Here's the background. Ungar points out that in July of 1798, Congress passed "An Act for the Relief of Sick and Disabled Seaman," which was signed by President Adams.
That law authorized the creation of a government operated system of marine hospitals and mandated that laboring merchant marine sailors pay a tax to support it.
Ungar argues that this blows away the argument made by many opponents of the individual mandate: That it's unconstitutional to mandate that all citizens purchase health
coverage, or that this violates the founding fathers' view of the proper role of government. Read more
- The Volokh Conspiracy opposing view

Treaties of the United States are the Supreme Law of the Land
Everyone has the right to a standard of living adequate for the health and well-being of himself and of his family, Article 25 - Universal Declaration of Human Rights, UDHR.
Treaties of the United States are the Supreme Law of the Land
Article VI, Clause 2 of the U.S. Constitution, the Supremacy Clause, which explicitly states that a ratified treaty is the Supreme Law of the land and all state law provisions which conflict with the treaty are overridden by the treaty.
This Constitution, and the Laws of the United States which shall be made in Pursuance thereof; and all Treaties made, or which shall be made, under the Authority of the
United States, shall be the supreme Law of the Land; and the Judges in every State shall be bound thereby, any Thing in the Constitution or Laws of any state to the Contrary
notwithstanding.
Article 25 Universal Declaration of Human Rights - UDHR
(1) Everyone has the right to a standard of living adequate for the health and well-being of himself and of his family, including food, clothing,
housing and medical care and necessary social services, and the right to security in the event of unemployment, sickness, disability, widowhood, old age or other lack of livelihood in circumstances
beyond his control.
(2) Motherhood and childhood are entitled to special care and assistance. All children, whether born in or out of wedlock, shall enjoy the same social
protection.
Also on the U.S. State Department website, Universal
Declaration of Human Rights (UDHR) Resolution 217(A)(III) of the United Nations General Assembly, December 10, 1948

FRONTLINE Sick Around The World

Introduction, April 15, 2008
In Sick Around the World, FRONTLINE teams up with veteran Washington Post foreign correspondent T.R. Reid to find out how five other capitalist democracies -- the United Kingdom, Japan, Germany, Taiwan and Switzerland -- deliver health care, and what the United States might learn from their successes and their failures. Read more
Five Capitalist Democracies & How They Do It
United Kingdom: Capitalist Democracy How They Do It
 Click for interview with expert on UK health system
Click for interview with expert on UK health system
Percentage of Gross Domestic Product (GDP) spent on health care: 8.3
Average family premium: None; funded by taxation.
Co-payments: None for most services; some co-pays for dental care, eyeglasses and 5 percent of prescriptions. Young people and the elderly are exempt from all drug co-pays.
What is it? The British system is "socialized medicine" because the government both provides and pays for health care. Britons pay taxes for health care, and the government-run National Health Service (NHS) distributes those funds to health care providers. Hospital doctors are paid salaries. General practitioners (GPs), who run private practices, are paid based on the number of patients they see. A small number of specialists work outside the NHS and see private-pay patients.
How does it work? Because the system is funded through taxes, administrative costs are low; there are no bills to collect or claims to review. Patients have a "medical home" in their GP, who also serves as a gatekeeper to the rest of the system; patients must see their GP before going to a specialist. GPs, who are paid extra for keeping their patients healthy, are instrumental in preventive care, an area in which Britain is a world leader.
What are the concerns? The stereotype of socialized medicine -- long waits and limited choice -- still has some truth. In response, the British government has instituted reforms to help make care more competitive and give patients more choice. Hospitals now compete for NHS funds distributed by local Primary Care Trusts, and starting in April 2008 patients are able to choose where they want to be treated for many procedures. Read more
Japan: Capitalist Democracy & How They Do It
 Click for interview with expert on the Japan system
Click for interview with expert on the Japan system
Percentage of GDP spent on health care: 8
Average family premium: $280 per month, with employers paying more than half.
Co-payments: 30 percent of the cost of a procedure, but the total amount paid in a month is capped according to income.
What is it? Japan uses a "social insurance" system in which all citizens are required to have health insurance, either through their work or purchased
from a nonprofit, community-based plan. Those who can't afford the premiums receive public assistance. Most health insurance is private; doctors and almost all hospitals are in the private
sector.
How does it work? Japan boasts some of the best health statistics in the world, no doubt due in part to the Japanese diet and lifestyle. Unlike the
U.K., there are no gatekeepers; the Japanese can go to any specialist when and as often as they like. Every two years the Ministry of Health negotiates with physicians to set the price for every
procedure. This helps keeps costs down.
What are the concerns? In fact, Japan has been so successful at keeping costs down that Japan now spends too little on health care; half of the
hospitals in Japan are operating in the red. Having no gatekeepers means there's no check on how often the Japanese use health care, and patients may lack a medical home. Read more
Germany: Capitalist Democracy & How They Do It
 click for interview
click for interview
Percentage of GDP spent on health care: 10.7
Average family premium: $750 per month; premiums are pegged to patients' income.
Co-payments: 10 euros ($15) every three months; some patients, like pregnant women, are exempt.
What is it? Germany, like Japan, uses a social insurance model. In fact, Germany is the birthplace of social insurance, which dates back to Chancellor
Otto von Bismarck. But unlike the Japanese, who get insurance from work or are assigned to a community fund, Germans are free to buy their insurance from one of more than 200 private, nonprofit
"sickness funds." As in Japan, the poor receive public assistance to pay their premiums.
How does it work? Sickness funds are nonprofit and cannot deny coverage based on preexisting conditions; they compete with each other for members, and
fund managers are paid based on the size of their enrollments. Like Japan, Germany is a single-payment system, but instead of the government negotiating the prices, the sickness funds bargain with
doctors as a group. Germans can go straight to a specialist without first seeing a gatekeeper doctor, but they may pay a higher co-pay if they do.
What are the concerns? The single-payment system leaves some German doctors feeling underpaid. A family doctor in Germany makes about two-thirds as much
as he or she would in America. (Then again, German doctors pay much less for malpractice insurance, and many attend medical school for free.) Germany also lets the richest 10 percent opt out of the
sickness funds in favor of U.S.-style for-profit insurance. These patients are generally seen more quickly by doctors, because the for-profit insurers pay doctors more than the sickness funds.
Read more
Taiwan: Capitalist Democracy & How They Do It
 click for interview
click for interview
Percentage GDP spent on health care: 6.3
Average family premium: $650 per year for a family for four.
Co-payments: 20 percent of the cost of drugs, up to $6.50; up to $7 for outpatient care; $1.80 for dental and traditional Chinese medicine. There are
exemptions for major diseases, childbirth, preventive services, and for the poor, veterans, and children.
What is it? Taiwan adopted a "National Health Insurance" model in 1995 after studying other countries' systems. Like Japan and Germany, all citizens
must have insurance, but there is only one, government-run insurer. Working people pay premiums split with their employers; others pay flat rates with government help; and some groups, like the poor
and veterans, are fully subsidized. The resulting system is similar to Canada's -- and the U.S. Medicare program.
How does it work? Taiwan's new health system extended insurance to the 40 percent of the population that lacked it while actually decreasing the growth
of health care spending. The Taiwanese can see any doctor without a referral. Every citizen has a smart card, which is used to store his or her medical history and bill the national insurer. The
system also helps public health officials monitor standards and effect policy changes nationwide. Thanks to this use of technology and the country's single insurer, Taiwan's health care system has
the lowest administrative costs in the world.
What are the concerns? Like Japan, Taiwan's system is not taking in enough money to cover the medical care it provides. The problem is compounded by
politics, because it is up to Taiwan's parliament to approve an increase in insurance premiums, which it has only done once since the program was enacted. Read more
Switzerland: Capitalist Democracy & How They Do It
 click for interview
click for interview
Percentage of GDP spent on health care: 11.6
Average monthly family premium: $750, paid entirely by consumers; there are government subsidies for low-income citizens.
Co-payments: 10 percent of the cost of services, up to $420 per year.
What is it? The Swiss system is social insurance like in Japan and Germany, voted in by a national referendum in 1994. Switzerland didn't have far to go
to achieve universal coverage; 95 percent of the population already had voluntary insurance when the law was passed. All citizens are required to have coverage; those not covered were automatically
assigned to a company. The government provides assistance to those who can't afford the premiums.
How does it work? The Swiss example shows that universal coverage is possible, even in a highly capitalist nation with powerful insurance and
pharmaceutical industries. Insurance companies are not allowed to make a profit on basic care and are prohibited from cherry-picking only young and healthy applicants. They can make money on
supplemental insurance, however. As in Germany, the insurers negotiate with providers to set standard prices for services, but drug prices are set by the government.
What are the concerns? The Swiss system is the second most expensive in the world -- but it's still far cheaper than U.S. health care. Drug prices are
still slightly higher than in other European nations, and even then the discounts may be subsidized by the more expensive U.S. market, where some Swiss drug companies make one-third of their profits.
In general, the Swiss do not have gatekeeper doctors, although some insurance plans require them or give a discount to consumers who use them. Read more
Public health-care in the People’s Republic of China

Healthcare in China
Wikipedia
Healthcare in China consists of both public and private medical institutions and insurance programs. About 95% of the population has at least basic health insurance coverage. Despite this, public health insurance generally only covers about half of medical costs, with the proportion lower for serious or chronic illnesses. Under the "Healthy China 2020" initiative, China is currently undertaking an effort to cut healthcare costs, and the government requires that insurance will cover 70% of costs by 2017.[1][2][2] The Chinese government is working on providing affordable basic healthcare to all residents by 2020.[3]
China has also become a major market for health-related multinational companies. Companies such as AstraZeneca, GlaxoSmithKline, Eli Lilly, and Merck entered the Chinese market and have experienced explosive growth. China has also become a growing hub for health care research and development.[4]
The above applies to Mainland China. Taiwan and the Special Administrative Regions of Hong Kong and Macau maintain their own separate universal healthcare systems. Read more

Affiliated Hospital of Medical College
Qingdao University, 16 Jiangsu Road
Qingdao, Shandong 266003, People’s Republic of China

Healthcare in Canada
Wikipedia
Health care in Canada is delivered through a publicly funded health care system, informally called Medicare, which is mostly free at the point of use and has most services provided by private entities.[2] It is guided by the provisions of the Canada Health Act of 1984.[3]
Current status
The government attempts to ensure the quality of care through federal standards. The government does not participate in day-to-day care or collect any information about an individual's health, which remains confidential between a person and their physician.[4] Canada's provincially based Medicare systems are cost-effective partly because of their administrative simplicity. In each province, each doctor handles the insurance claim against the provincial insurer. There is no need for the person who accesses healthcare to be involved in billing and reclaim. Private health expenditure accounts for 30% of health care financing.[5] The Canada Health Act does not cover prescription drugs, home care or long-term care, prescription glasses or dental care, which means most Canadians pay out-of-pocket for these services or rely on private insurance.[4] Provinces provide partial coverage for some of these items for vulnerable populations (children, those living in poverty and seniors).[4] Limited coverage is provided for mental health care.
Competitive practices such as advertising are kept to a minimum, thus maximizing the percentage of revenues that go directly towards care. In general, costs are paid through funding from income taxes. In British Columbia, taxation-based funding is supplemented by a fixed monthly premium which is waived or reduced for those on low incomes.[6] There are no deductibles on basic health care and co-pays are extremely low or non-existent (supplemental insurance such as Fair Pharmacare may have deductibles, depending on income). In general, user fees are not permitted by the Canada Health Act, though some physicians get around this by charging annual fees for services which include non-essential health options, or items which are not covered by the public plan, such as doctors notes, prescription refills over the phone.[4] Read more

The New England Journal of Medicine
Private Health Care in Canada
by Robert Steinbrook, M.D.
N Engl J Med 2006; 354:1661-1664
The hallmarks of Canada's government-funded universal health care system include the public provision of core physician and hospital services and the absence of
copayments and other patient charges.1 The system is often championed as a reflection of Canadian values and as an alternative that the United States might emulate. In 2003, Canada's health care
spending per capita was $3,003 — higher than that of some European countries and Japan but about half that of the United States (see tableHealth Care Statistics for Canada and Other Countries.).
Canada's spending as a proportion of gross domestic product has remained steady, while many other countries have been spending an increasing proportion on health care. Now, however, Canada's system,
called Medicare, is under attack for inefficiency, insufficient funding, and failure to meet some patients' needs in a timely fashion. Read more
The New England Journal of Medicine, Facebook

Canada's Supreme Court Chips Away at National Health Care
The New York Times
By CLIFFORD KRAUSS
Published: June 9, 2005
TORONTO, June 9 - The Canadian Supreme Court struck down a Quebec law banning private medical insurance today, dealing an acute blow to the publicly financed national
health care system.
The court stopped short of striking down the constitutionality of the country's vaunted nationwide coverage, but legal experts said the ruling would open the door to a
wave of lawsuits challenging the health care system in other provinces.
The system, providing Canadians with free doctor's services that are paid for by taxes, has generally been supported by the public, and is broadly identified with the
Canadian national character. Read more

Health care in Mexico
Wikipedia
Healthcare in Mexico is provided via public institutions, private entities, or private physicians. Healthcare delivered through private organizations
operates entirely on the free-market system, i.e., it is available to those who can afford it. This is also the case of
healthcare obtained from private physicians at their private office or clinic. Public healthcare delivery, on the other hand, is accomplished via an elaborate provisioning and delivery system put in
place by the Mexican Federal Government. In 2012, Mexico instituted universal healthcare.[1] As of December 31, 2013, there were 4,466 hospitals in Mexico.[2] Read more

Healthcare in Cuba
Wikipedia
The Cuban government operates a national health system and assumes fiscal and administrative responsibility for the health care of all its citizens.[1] There are no private hospitals or clinics as all health services are government-run. The present Minister for Public Health is Roberto Morales Ojeda.
Like the rest of the Cuban economy, Cuban medical care suffered following the end of Soviet subsidies in 1991; the stepping up of the US embargo against Cuba at this time also had an effect.[2]
Having practiced medicine for over 30 years, Congressman Paul gives his perspective on the past and future of medicine in this country, and the effects of government and special interests on quality, costs and access.
Chefs, Butlers, Marble Baths: Hospitals Vie for Affluent
 Nancy Hemenway in the library of Mount Sinai Medical Center's Eleven West wing, where the best room costs $1,600 a day
Nancy Hemenway in the library of Mount Sinai Medical Center's Eleven West wing, where the best room costs $1,600 a day

Chefs, Butlers, Marble Baths: Hospitals Vie for the Affluent
The New York Times
By NINA BERNSTEIN
January 21, 2012
The feverish patient had spent hours in a crowded emergency room. When she opened her eyes in her Manhattan hospital room last winter, she recalled later, she wondered
if she could be hallucinating: "This is like the Four Seasons — where am I?"
The bed linens were by Frette, Italian purveyors of high-thread-count sheets to popes and princes. The bathroom gleamed with polished marble. Huge windows displayed
panoramic East River views. And in the hush of her $2,400 suite, a man in a black vest and tie proffered an elaborate menu and told her, "I’ll be your butler."
It was Greenberg 14 South, the elite wing on the new penthouse floor of NewYork-Presbyterian/Weill Cornell hospital. Pampering and décor to rival a grand hotel, if not a
Downton Abbey, have long been the hallmark of such "amenities units," often hidden behind closed doors at New York’s premier hospitals. But the phenomenon is escalating here and around the country,
health care design specialists say, part of an international competition for wealthy patients willing to pay extra, even as the federal government cuts back hospital reimbursement in pursuit of a
more universal and affordable American medical system.
"It’s not just competing on medical grounds and specialties, but competing for customers who can go just about anywhere," said Helen K. Cohen, a specialist in health
facilities at the international architectural firm HOK, which recently designed luxury hospital floors in Singapore and London and renovated NewYork-Presbyterian’s elite offerings in the McKeen
Pavilion in Washington Heights. "These kinds of patients, they’re paying cash — they’re the best kind of patient to have," she added. "Theoretically, it trickles down."
A waterfall, a grand piano and the image of a giant orchid grace the soaring ninth floor atrium of McKeen, leading to refurbished rooms that, like those in the
hospital’s East 68th Street penthouse, cost patients $1,000 to $1,500 a day, and can be combined. That fee is on top of whatever base rate insurance pays to the hospital, or the roughly $4,500 a day
that foreigners are charged, according to the hospital’s international services department.
But in the age of Occupy Wall Street, catering to the rich can be trickier than ever, noted Avani Parikh, who worked for NewYork-Presbyterian as in-house project leader
when the 14th floor was undertaken. She pointed to the recent ruckus at Lenox Hill Hospital, where parents with newborns in the intensive-care unit complained that security guards had restricted
their movements and papered over hospital security cameras in their zeal to please Jay-Z (real name Shawn Carter) and Beyoncé Knowles, whose daughter was born on Jan. 7 in a new "executive
suite."
 click on menu to enlarge
click on menu to enlarge
More Physicians Say No to Endless Workdays
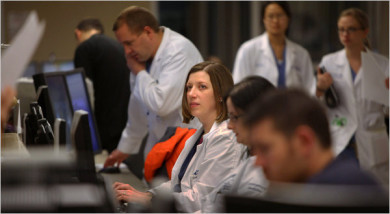 Dr. Kate Dewar, daughter of a doctor, chose work in an emergency room over private practice. Nicole Bengiveno/The New York Times
Dr. Kate Dewar, daughter of a doctor, chose work in an emergency room over private practice. Nicole Bengiveno/The New York Times

More Physicians Say No to Endless Workdays
The New York Times
by GARDINER HARRIS
April 1, 2011
HONESDALE, Pa. — Even as a girl, Dr. Kate Dewar seemed destined to inherit the small-town medical practice of her grandfather and father. At 4, she could explain how to
insert a pulmonary catheter. At 12, she could suture a gash. And when she entered medical school, she and her father talked eagerly about practicing together.
But when she finishes residency this summer, Dr. Dewar, 31, will not be going home. Instead, she will take a job as a salaried emergency room doctor at a hospital in
Elmira, N.Y., two hours away. An important reason is that she prefers the fast pace and interesting puzzles of emergency medicine, but another reason is that on Feb. 7 she gave birth to twins, and
she cannot imagine raising them while working as hard as her father did.
"My father tried really hard to get home, but work always got in the way," Dr. Dewar said. "Even on Christmas morning, we would have to wait to open our presents until
Dad was done rounding at the hospital."
Dr. Dewar’s change of heart demonstrates the significant changes in American medicine that are transforming the way patients get care.
For decades, medicine has been dominated by fiercely independent doctors who owned their practices, worked night and day, had comfortable incomes and rarely saw their
families.
But with two babies, Dr. Dewar wants a life different from her father’s and grandfather’s. So instead of being an entrepreneur, she will become an employee of a large
corporation working 36 hours a week — half the hours her father and grandfather worked.
High-end Medical Option Prompts Medicare Worries

High-end medical option prompts Medicare worries
Yahoo/Associated Press
April 2, 2011
Every year, thousands of people make a deal with their doctor: I'll pay you a fixed annual fee, whether or not I need your services, and in return you'll see me the day
I call, remember who I am and what ails me, and give me your undivided attention.
But this arrangement potentially poses a big threat to Medicare and to the new world of medical care envisioned under President Barack Obama's health
overhaul.
The spread of "concierge medicine," where doctors limit their practice to patients who pay a fee of about $1,500 a year, could drive a wedge among the insured.
Eventually, people unable to afford the retainer might find themselves stuck on a lower tier, facing less time with doctors and longer waits.
Medicare recipients, who account for a big share of patients in doctors' offices, are the most vulnerable. The program's financial troubles are causing doctors to
reassess their participation. But the impact could be broader because primary care doctors are in short supply and the health law will bring in more than 30 million newly insured
patients.
If concierge medicine goes beyond just a thriving niche, it could lead to a kind of insurance caste system. Read more
Talk Doesn’t Pay, So Psychiatry Turns to Drug Therapy
 "I had to train myself not to get too interested in their problems, and not to get sidetracked trying to be a semi-therapist." DR. DONALD LEVIN, a psychiatrist whose practice no longer includes talk therapy. Richard Perry/The New York Times
"I had to train myself not to get too interested in their problems, and not to get sidetracked trying to be a semi-therapist." DR. DONALD LEVIN, a psychiatrist whose practice no longer includes talk therapy. Richard Perry/The New York Times

Talk Doesn’t Pay, So Psychiatry Turns Instead to Drug Therapy
The New York Times
by GARDINER HARRIS
March 5, 2011
DOYLESTOWN, Pa. — Alone with his psychiatrist, the patient confided that his newborn had serious health problems, his distraught wife was screaming at him and he had
started drinking again. With his life and second marriage falling apart, the man said he needed help.
But the psychiatrist, Dr. Donald Levin, stopped him and said: "Hold it. I’m not your therapist. I could adjust your medications, but I don’t think that’s
appropriate."
Like many of the nation’s 48,000 psychiatrists, Dr. Levin, in large part because of changes in how much insurance will pay, no longer provides talk therapy, the form of
psychiatry popularized by Sigmund Freud that dominated the profession for decades. Instead, he prescribes medication, usually after a brief consultation with each patient. So Dr. Levin sent the man
away with a referral to a less costly therapist and a personal crisis unexplored and unresolved.
Medicine is rapidly changing in the United States from a cottage industry to one dominated by large hospital groups and corporations, but the new efficiencies can be
accompanied by a telling loss of intimacy between doctors and patients. And no specialty has suffered this loss more profoundly than psychiatry.
Trained as a traditional psychiatrist at Michael Reese Hospital, a sprawling Chicago medical center that has since closed, Dr. Levin, 68, first established a private
practice in 1972, when talk therapy was in its heyday.
Then, like many psychiatrists, he treated 50 to 60 patients in once- or twice-weekly talk-therapy sessions of 45 minutes each. Now, like many of his peers, he treats
1,200 people in mostly 15-minute visits for prescription adjustments that are sometimes months apart. Then, he knew his patients’ inner lives better than he knew his wife’s; now, he often cannot
remember their names. Then, his goal was to help his patients become happy and fulfilled; now, it is just to keep them functional.
Dr. Levin has found the transition difficult. He now resists helping patients to manage their lives better. "I had to train myself not to get too interested in their
problems," he said, "and not to get sidetracked trying to be a semi-therapist." Read more
Talk Doesn’t Pay, So Psychiatry Turns In[...]
Adobe Acrobat document [49.4 KB]
Nuns, a ‘Dying Breed,’ Fade From Leadership Roles at Catholic Hospitals
 "We can't be maudlin about this," Sister Mary Jean Ryan said of the changing situation for nuns. Sid Hastings for The New York Times
"We can't be maudlin about this," Sister Mary Jean Ryan said of the changing situation for nuns. Sid Hastings for The New York Times
 The Franciscan Sisters of Mary, St. Louis 1872, later ministered to patients in hospitals
The Franciscan Sisters of Mary, St. Louis 1872, later ministered to patients in hospitals
Nuns, a ‘Dying Breed,’ Fade From Leadership Roles at Catholic Hospitals
The New York Times
by KEVIN SACK
August 20, 2011
ST. LOUIS — When Sister Mary Jean Ryan entered the convent as a young nurse in 1960, virtually every department of every Catholic hospital was run by a nun, from
pediatrics to dietary to billing. After her retirement on July 31 as the chief executive of one of the country’s largest networks of Catholic hospitals, only 11 nuns remained among her company’s more
than 22,000 employees, and none were administrators.
For SSM Health Care, a $4.2 billion enterprise that evolved from the work of five German nuns who arrived here in 1872, Sister Mary Jean’s departure after 25 years as
the company’s first chief executive marks a poignant passing. The gradual transition from religious to lay leadership, which has been changing the face of Catholic health care for decades, is now
nearly complete.
In 1968, nuns or priests served as chief executives of 770 of the country’s 796 Catholic hospitals, according to the Catholic Health Association. Today, they preside
over 8 of 636 hospitals. With Sister Mary Jean’s departure, only 8 of 59 Catholic health care systems are directed by religious executives.
SSM, which is now led by William P. Thompson, a Catholic layman and longtime company executive, had been the largest Catholic health system still managed by a nun.
Formed in 1986, the St. Louis firm consolidated the management of 15 Catholic hospitals and two nursing homes in Missouri, Illinois, Oklahoma and Wisconsin.
As with other healing orders that have ceded control, the Franciscan Sisters of Mary prepared for their inevitable detachment from SSM with more planning than
sentiment.
"We can’t be maudlin about this," said Sister Mary Jean, 73, who still presides over the company’s board. "I mean, yes, we are a dying breed. We are disappearing from
the face of the earth and all of that. That being said, perhaps this is a moment for people to acknowledge the contribution that has been made by women religious throughout our history in the United
States."
The leadership shift has stirred angst in many Catholic hospitals about whether the values imparted by the nuns, concerning the treatment of both patients and employees,
can withstand bottom-line forces without their day-to-day vigilance. Although their influence is often described as intangible, the nuns kept their hospitals focused on serving the needy and brought
a spiritual reassurance that healing would prevail over profit, authorities on Catholic health care say.
In the case of SSM, that has meant turning away business arrangements with doctors who decline to accept Medicaid. It has meant discounting treatment for the poor and
offering charity care to the uninsured, just as the order’s founders did. The St. Louis nuns’ earliest ledgers denoted patients unable to pay as "Our dear Lord’s." Read more
 www.pnhp.org/news/2014/october/dr-martin-luther-king-on-health-care-injustice
www.pnhp.org/news/2014/october/dr-martin-luther-king-on-health-care-injustice